The moderator for this website spent several hours reviewing the IARC Monograph that consists of 480 pages in the full PDF document version. Important observations and conclusions were extracted from that document in an attempt to create a synopsis that included all the key points. The synopsis, once compiled, consisted of 12 typed pages. That synopsis was then pasted into this webage. In creating the synopsis, no words were changed from the original document but sections were reformatted and some sentences were either underscored or placed in bold print in order to further highlight key words or conclusions. All of what follows should be considered exact quotations.
Rather than reading the synopsis, if you prefer to read the entire document, here is a link for the entire Monograph:
IARC Monograph Vol. 102, for Non-Ionizing Radiation, Part 2: Radiofrequency Electromagnetic Fields
[Several months after the initial release of the IARC Monograph, a final published version was released which resulted in a new cover and a change in page numbers from the original version released in April 2013:
IARC Monograph Volume 102 (Final Published Version)]
General Remarks
The topic of this Monograph is the evaluation of the carcinogenicity of radiation in the radiofrequency (RF) range (30 kHz to 300 GHz) of the electromagnetic spectrum. This type of radiation is emitted by devices used in wireless telecommunication, including mobile phones, and by many other sources in occupational and general environmental settings. Exposures are ubiquitous in more developed countries and rapidly increasing in the developing world, in particular with respect to the use of mobile phones. There is rising concern as to whether exposure to RF radiation emitted by a mobile phone affects human health and, specifically, whether mobile-phone use increases the risk of cancer of the brain. The general public, manufacturers, regulatory authorities and public health agencies are seeking evidence on the safety of mobile-phone use. Consequently, there has been intense interest in the development and outcome of this IARC Monograph. This interest reflects the high prevalence of exposure (which increasingly extends to children), the vast scope of the telecommunications industry, the findings of some epidemiological studies that suggest an increased risk of cancer, and a high level of media coverage of the topic of mobile phones and cancer. Although the preparation of this Monograph had been scheduled so as to include the results of the large international case–control study INTERPHONE on mobile-phone use (conducted in 2000–2004; published in 2010), it should be emphasized that the evaluations in this volume address the general question of whether RF radiation causes cancer in humans or in experimental animals: it does not specifically or exclusively consider mobile phones, but rather the type of radiation emitted by mobile phones and various other sources. Furthermore, this Monograph is focused on the potential for an increased risk of cancer among those exposed to RF radiation, but does not provide a quantitative assessment of any cancer risk, nor does it discuss or evaluate any other potential health effects of RF radiation.
The Working Group agreed to consider three categories of human exposure to RF radiation: (a) environmental sources such as mobile-phone base stations, broadcast antennae, smart meters, and medical applications; (b) occupational sources such as high-frequency dielectric and induction heaters, and high-power pulsed radars; and (c) the use of personal devices such as mobile phones, cordless phones, Bluetooth devices, and amateur radios.
The general population receives the highest exposure from transmitters close to the body, including hand-held devices such as mobile phones, which deposit most of the RF energy in the brain. Holding a mobile phone to the ear to make a voice call can result in high specific rates of absorption (SAR) of RF energy in the brain, depending on the design and position of the phone and its antenna in relation to the head, the anatomy of the head, and the quality of the connection with the base-station antenna: the better the connection, which is ensured by a dense network of base stations, the lower the energy output from the phone. In children using mobile phones, the average deposition of RF energy may be two times higher in the brain and up to ten times higher in the bone marrow of the skull than in adult users. The use of hands-free kits lowers exposure of the brain to less than 10% of the exposure from use at the ear, but it may increase exposure to other parts of the body.
Epidemiological evidence of an association between RF radiation and cancer comes from time-trend, cohort, and case–control studies. The populations in these studies were exposed to RF radiation in occupational settings, from sources in the general environment, and from use of wireless (mobile and cordless) phones. Two sets of data from case–control studies were considered by the Working Group as the principal and most informative basis for their evaluation of the human evidence, i.e. the INTERPHONE study and the Swedish case–control studies; both sets of data focused on brain tumours among mobile-phone users.
The Working Group reviewed a large number of studies with end-points relevant to mechanisms of carcinogenesis, including genotoxicity, effects on immune function, gene and protein expression, cell signalling, oxidative stress, and apoptosis. Studies on the possible effects of RF radiation on the blood–brain barrier, and on a variety of effects in the brain itself were also considered. The Working Group found several studies inadequately controlled for the thermal effects of RF radiation, but also noted well conducted studies showing aneuploidy, spindle disturbances, altered microtubule structures or induction of DNA damage. While RF radiation has insufficient energy to directly produce genetic damage, other changes such as induction of oxidative stress and production of reactive oxygen species may explain these results. Indeed, several studies in vitro evaluated the possible role of RF radiation in altering levels of intracellular oxidants or activities of antioxidant enzymes. While the overall evidence was inconclusive, the Working Group expressed concern about the results from several of these studies.
Sources of Exposure
Personal Exposure
The general community can come into contact with several potentially important sources of RF radiation as part of their personal life, involving some degree of choice, including use of a mobile phone, other communication technologies, or household devices.
Exposure from Mobile Phones
With continuing changes in technology, use of mobile phones has become widespread over the last two decades. As a result, the population exposed to RF radiation has greatly increased and is still expanding, with more and more children among its number. Over these two decades, there has been rising concern regarding the potential health risks associated with use of mobile phones, particularly the possibility of increased risk of cancer of the brain. These concerns have stimulated a diverse programme of research, including epidemiological studies carried out to assess the association of mobile-phone use with risk of cancer of the brain and other diseases. The strength of epidemiological studies is obviously the capacity to directly assess the risks associated with use of mobile phones in the general population; however, the observations collected in these studies clearly only address the various exposure scenarios that existed up to the time of observation. Thus the studies carried out to date include few participants who have used mobile phones for > 10–15 years. Any risks that might be associated with lengthier exposure or with a longer interval since first exposure would not be captured by existing studies.
Three types of study design have been applied to address the question whether an increased risk of cancer is associated with RF emitted by mobile phones. These are ecological studies (in particular, observations of time trends in disease rates), case–control studies, and cohort studies. The strengths and limitations of each of these designs in general have been well described. Here, the Working Group focused on the characteristics of these designs as applied to the investigation of the potential risks of mobile-phone use.
DECT Phones
Another important source of personal RF exposure is the home use of DECT phones, which have been replacing traditional handsets in the home. As the DECT base-station is within the home and at most some tens of metres from the handset, the average power generated by the DECT phone is less than that of a mobile phone, where the base station may be up to some kilometers away. However, the power output of a DECT base station in close proximity to a person may be comparable to that of a 3G phone, so proximity to a DECT phone base-station should be taken into account when estimating RF exposure in epidemiological studies in which sizeable numbers of subjects have used 3G phones. A recent study of Australian schoolchildren found that 87% had a DECT phone at home, and although there was only a weak correlation (r = 0.38) between mobile-phone and DECT phone use, this suggests that DECT-phone use needs to be considered in the assessment of RF exposure (Redmayne et al., 2010).
Other Communication Technologies and Domestic Sources
Within homes there are many other potential sources of RF exposure, including baby monitors, microwave ovens, Wi-Fi, Bluetooth, various types of radios and remote-controlled toys. A study of 226 households in lower Austria measured the peak power of emitted bursts of RF exposure from each of these types of devices in bedrooms, where the residents spend the most time in one position. The highest peak RF values were measured for mobile-phone and DECT base stations in the 2400-MHz band (Tomitsch et al., 2010).
Wireless Networks
Wireless networking has developed rapidly since about 2000 and is becoming the method of choice for connecting mobile devices such as laptop computers and mobile phones to other electronic systems and to the Internet. The networks are found in homes, schools, public places such as cafes and transport hubs, and in the workplace. The systems operate to the IEEE802.11 family of technical standards and are often known as “Wi-Fi,” after the Wi-Fi Alliance, an organization that certifies inter-operability of devices on the market.
The RF emissions from Wi-Fi devices are in the form of short bursts containing portions of the data being transmitted and other information, such as acknowledgements that data have been successfully received. Unlike the emissions from mobile phones using TDMA, the bursts are irregular in terms of timing and duration. Typical bursts range from about 10 μs to about 1 ms in duration. If data are lost or corrupted during transmission, bursts are retransmitted until they are successfully received. Also, under conditions where communications are poor, e.g. due to weak signal strength, the systems can lower their data-transfer rates to have better signal-to-noise ratios and improved reliability.
This increases the cumulative time that it takes to transmit a given amount of data. Thus, high signal strengths from Wi-Fi devices (during transmission of bursts) do not necessarily translate to higher exposures, because this results in lower duty factors (Mann, 2010). Comprehensive data are yet to be published regarding the duty factors of Wi-Fi equipment during normal use; however, Khalid et al. (2011) has reported initial results from the use of data traffic capturing and packet-counting equipment in school networks. Transmitted bursts were captured to determine the proportion of time during which Wi-Fi devices transmitted while children were using laptops during their lessons. The laptops were mostly used for receiving traffic from the access points and therefore laptop transmit times were low. Duty factors for the monitored laptops were consistently less than 1% and those of access points were less than 10%. Baseline duty factors of access points (with no data being transferred) are about 1%, due to beacon pulses of duration 1 ms that are produced at a rate of ten pulses per second (Mann, 2010).
Domestic Sources
There are few powerful sources of RF in the home; however, among these, induction cooking hobs and microwave ovens are of note. Less powerful sources include remote-controlled toys, baby monitors, and the mobile/cordless phones and the Wi-Fi systems described earlier.
Microwave ovens are standard fixtures in many homes and contain microwave sources operating at a frequency of 2.45 GHz and producing powers between 500 W and 2 kW. The design of such ovens is such that leakage is kept to a minimum and a product-performance technical standard requires that microwave-power density levels fall below 50 W/m2 at a distance of 5 cm. Several large surveys of leakage levels have been performed, as described in ICNIRP (2009a), and these indicate that approximately 99% of ovens comply with the emission limit. According to the measurements of Bangay & Zombolas (2003), the maximum local SAR values at the emission limit are 0.256 W/kg and the maximum 10 g averaged SAR is 0.0056 W/kg.
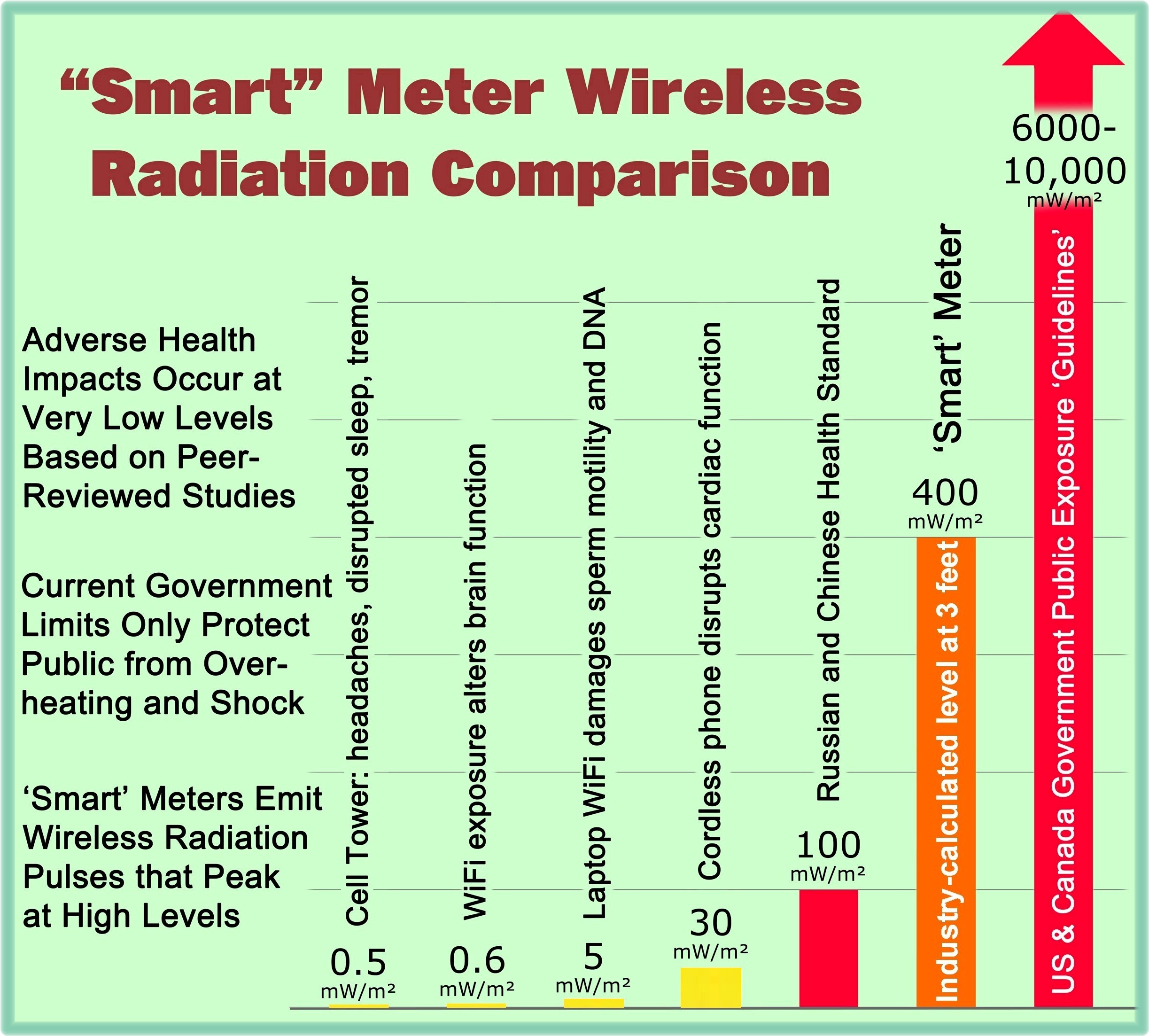
A new source of RF that is currently being introduced and that seems set to enter many homes is the transmitter associated with “smart” metering of electricity consumption and potentially metering for other services such as water and gas. There is no global approach to gathering information from smart meters and relaying it back to the utility companies, but it is clear that radio communications will be involved. Some systems may use mobile-phone networks for this purpose, while others may use dedicated radio infrastructures. Some systems may also involve a home area network (HAN) within which individual electrical devices in the home can relay information about usage to a central collection point, allowing residents to examine the information and make decisions about their energy consumption. Two recent investigations commissioned by the Electric Power Research Institute (available on the EPRI webpage) suggest that the power level of radio transmissions will be similar to that of mobile phones, but that the duty factors will be low (on average, such devices will transmit for a small proportion of time only). Low duty factors, combined with the greater distances of these devices from people compared with mobile phones, imply that exposures will be low when compared with exposure guidelines.
Interaction of RF-EMF with Biological Systems
Conclusion
In conclusion, tissue heating is the best established mechanism for RF radiation-induced effects in biological systems. However, there are also numerous reports of specific biological effects from modulated RF-EMF, particularly low-frequency modulated fields. Mechanistic studies will be needed to determine how effects that are reproducible might be occurring, e.g. via the induction of reactive oxygen species, induction of ferromagnetic resonance, demodulation of pulsed RF signals, or alteration of ligand binding to hydrophobic sites in receptor proteins. Although it has been argued that RF radiation cannot induce physiological effects at exposure intensities that do not cause an increase in tissue temperature, it is likely that not all mechanisms of interaction between weak RF-EMF (with the various signal modulations used in wireless communications) and biological structures have been discovered or fully characterized. Biological systems are complex and factors such as metabolic activity, growth phase, cell density, and antioxidant level might alter the potential effects of RF radiation. Alternative mechanisms will need to be considered and explored to explain consistently observed RF-dependent changes in controlled studies of biological exposure. While the debate continues on whether or not non-thermal biological effects occur as a result of exposures to low-intensity RF radiation, it may be difficult to specify observed effects as non-thermal because of the high sensitivities of certain physiological responses to small increases in temperature.
Genetic and Related Effects
[The Working Group noted that while several studies showed positive responses at high SAR values, some of these were due to thermal effects. The Working Group concluded that there was weak evidence that exposure to RF radiation is genotoxic in experimental systems in mammalian and non-mammalian cells in vitro.]
Effects of Low-level Exposure to RF Radiation on the Immune System
[The Working Group noted that studies of humans exposed to RF radiation provided weak evidence for effects on the humoral immune system.]
Effects of Exposure to RF Radiation on Gene and Protein Expression
[Of the numerous studies that investigated the potential for RF radiation to modify genetranscription and protein-expression levels in a variety of animal models in vivo and human models in vitro, some reported effects under conditions where the possibility of thermal confounding could not be excluded. Other studies reported alterations in gene/protein expression under non-thermal exposure conditions, but typically in single, usually unreplicated experiments, or under experimental conditions with methodological shortcomings. There were no studies in human populations. Overall, there was weak evidence that exposure to RF radiation affects gene and protein expression.]
Other Relevant Effects
[The Working Group concluded that there is weak evidence that RF radiation affects apoptosis in mammalian cells.]
Dose and Duration of Exposure
While accumulated absorbed energy is measured as “dose” (dose rate multiplied by exposure time) in radiobiology, guidelines for exposures to RF radiation usually state power density or SAR (dose rate analogue) to define exposure. Several studies have analysed the relationship between dose and duration of exposure, with results suggesting that duration of exposure and dose may be important for cancer-relevant effects. In particular, prolonging the duration of exposure could compensate for the effects of a reduction in intensity.
Exposure Data
This Monograph is concerned with nonionizing radiation in the radiofrequency (RF) range of the electromagnetic spectrum, i.e. between 30 kHz and 300 GHz. The corresponding wavelengths – the distance between successive peaks of the RF waves – range from 10 km to 1 mm, respectively. Human exposure to RF radiation can occur from many different sources and under a wide variety of circumstances, including the use of personal devices (mobile phones, cordless phones, Wi-Fi, Bluetooth, amateur radios, etc.), occupational sources (high-frequency dielectric and induction heaters, broadcast antennas, high-power pulsed radars, and medical applications), and environmental sources (mobile phone base stations, broadcast antennae). These multiple sources contribute to an individual’s total exposure, with contributions varying by different characteristics, e.g. place of residence. The dominant sources of human exposure to RF radiation are near-field sources for workers, and transmitters operating on or in close vicinity to the body, such as hand-held devices, for the general population.
Electromagnetic fields generated by RF sources couple with the human body, which results in induced electric and magnetic fields and associated currents inside body tissues. The most important factor that determines exposure is the distance of the transmitter from the human body, within the main radiation beam. In a first approximation, the induced field strength is proportional to the time-averaged radiated power and inversely proportional to the distance from the source. In addition to distance, the efficiency of coupling and the resulting field distribution inside the body strongly depend on properties of the fields, such as frequency, polarization, distance from the antenna and direction of incidence, and on anatomical features of the exposed person, including height, posture, body mass index, shape of the head and associated structures such as the pinna (the outer ear), and dielectric properties of tissues. Induced fields within the body are highly non-uniform, with local hotspots and variations of several orders of magnitude.
Tissue heating is the most firmly established mechanism for effects of RF radiation in biological systems. Although it has been argued that RF radiation cannot induce physiological effects at exposure intensities that do not cause a detectable increase in tissue temperature, except for reactions mediated by free radical pairs, it is likely that not all mechanisms of interaction between weak RF fields, with the various signal modulations used in wireless communications, and biological structures have yet been discovered or fully characterized.
Human Carcinogenicity Data
The epidemiological evidence on possible associations of exposure to RF radiation with cancer comes from studies of diverse design that have assessed a range of sources of exposure: the populations included people exposed in occupational settings, people exposed through sources in the general environment, e.g. transmission towers, and people exposed through use of wireless (mobile and cordless) telephones. The most robust evidence is for mobile phones, the most extensively investigated exposure source.
As for any compilation of findings of epidemiological studies, interpretation of this evidence needs to give consideration to the possibility that observed associations reflect chance, bias, or confounding, rather than an underlying causal effect. The investigation of risk of cancer of the brain associated with mobile-phone use poses complex methodological challenges in the conduct of the research and in the analysis and interpretation of the findings.
Tumours of the Central Nervous System: Gliomas of the Brain
In summary, in the INTERPHONE study there was no increased risk of glioma associated with having ever been a regular user of mobile phones. However, there were indications of an increased risk of glioma at the highest levels of cumulative call time, for ipsilateral exposures, and for tumours in the temporal lobe, but chance or bias may explain this increased risk.
In 2011, Swedish investigators reported the findings of a pooled analysis of associations of mobile-phone and cordless-phone use and risk of glioma.
The Working Group noted several strengths of the study. It was the only study to assess exposure to cordless phones. By using registries for case ascertainment and population-based controls, and by achieving high response rates, the investigators minimized the potential for selection bias. However, the possibility of information bias cannot be excluded, and specific validation studies were not carried out in this population.
Overall, the Working Group reviewed all the available evidence with regard to the use of wireless phones, including both mobile and cordless phones, and the risk of glioma. Time trends were considered, as were several early case–control studies and one cohort study. The evidence from these studies was considered less informative than the results of the INTERPHONE study and the Swedish case–control study. While both of these are susceptible to bias, the Working Group concluded that these findings could not be dismissed as reflecting bias alone, and that a causal interpretation was possible.
Other Tumours of the Central Nervous System: Acoustic Neuroma
In considering the evidence on acoustic neuroma, the Working Group considered the same methodological concerns as for glioma, but concluded that bias was not sufficient to explain the positive findings, particularly those of the study from Sweden.
Occupational Exposure
In summary, while there were weak suggestions of a possible increase in risk of leukaemia or lymphoma associated with occupational exposure to RF radiation, the limited exposure assessment and possible confounding make these results difficult to interpret.
Environmental Exposure
The fourth study assessed proximity of subjects’ beds to base stations of DECT cordless phones in the home. It found a weak and imprecise increase in risk of brain cancer associated with sleeping near a base station. Another study found high risks for brain, breast and other cancers associated with the place of residence where the highest power density from a nearby base-station antenna was measured, but the results were imprecise and based on only a few cases. Together, these studies provide no indication that environmental exposure to RF radiation increases the risk of brain tumours.
Animal Carcinogenicity Data
Although the value of two of these studies was weakened by their unknown relevance to cancer in humans, the Working Group concluded that they did provide some additional evidence supporting the carcinogenicity of RF radiation in experimental animals.
Other Relevant Data
The data to evaluate the mechanisms by which RF radiation may cause or enhance carcinogenesis are extensive and diverse. Studies in humans from occupational cohorts, mobilephone users and controlled exposures in experimental settings provide information on effects in various tissues, including blood and brain. Studies in animals have been focused on a variety of organs and tissues. Assays in vitro in human cells, other mammalian cells, and cells from other organisms provide the largest set of data from which to evaluate mechanisms. Many studies were confounded by significant increases in the temperature of the cells, leading to thermal effects that could not be dissociated from nonthermal RF-induced changes. The conclusions presented in this section for results in vivo and in vitro pertain only to those studies for which the Working Group concluded that thermal confounding did not occur.
While RF radiation has insufficient energy to produce these types of direct genetic damage, other changes such as oxidative stress and production of reactive oxygen species may explain these results. The remaining few studies that gave positive results for genetic damage at lower doses could not be replicated after multiple attempts in different laboratories, raising serious questions regarding the original findings. A single study showing altered microtubule structures at low exposures remains a concern. Overall, the Working Group concluded that there was weak evidence that RF radiation is genotoxic, and no evidence for the mutagenicity of RF radiation.
Overall, the Working Group concluded that there was insufficient evidence to determine that alterations in immune function induced by exposure to RF radiation affect carcinogenesis in humans.
On the basis of the above considerations, the Working Group concluded that data from studies of genes, proteins and changes in cellular signalling show weak evidence of effects from RF radiation, but did not provide mechanistic information relevant to carcinogenesis in humans.
Other Mechanistic End-Points
Several potential changes resulting from exposure to RF radiation are summarized here. With the exception of changes in cerebral blood flow, many of the other studies reviewed by the Working Group provided conflicting, negative or very limited information, which made it difficult to draw conclusions, especially in relation to carcinogenesis. These studies focused on electrical activity in the brain, cognitive function, general sensitivity to RF radiation and alterations in brain biochemistry. Even though the relationship between alterations in cerebral blood flow during exposure to RF radiation cannot be directly related to carcinogenesis, the Working Group concluded that the available data were sufficiently consistent to identify them as important findings.
A few studies in human cells in vitro evaluated the possible role of exposure to RF radiation in altering levels of intracellular oxidants or activities of antioxidant enzymes. One study showed a marginal effect, while other studies demonstrated an increase in activity with increasing exposures. There were not enough studies to make a reasonable assessment of the consistency of these findings. Additional studies addressed this issue in in-vitro systems with non-human cells. While most of these did not find changes, one study evaluated the formation of DNA adducts from reactive oxygen species (8-hydroxy-deoxyguanosine) and was able to demonstrate reversal of this effect by melatonin. While the overall evidence was inconclusive, the results from in-vitro studies with animal models raise some concern.
Overall, the Working Group concluded that there was weak evidence that exposure to RF radiation affects oxidative stress and alters the levels of reactive oxygen species.
The evidence that exposure to RF radiation alters the blood–brain barrier was considered weak.
The evidence that exposure to RF radiation alters apoptosis was considered weak.
The evidence that RF radiation alters cellular replication was considered weak.
There was weak evidence from in-vitro studies that exposure to RF radiation alters ornithine decarboxylase activity. The evidence that exposure to RF radiation, at intensities below the level of thermal effects, may produce oxidative stress in brain tissue and may affect neural functions was considered weak.
Cancer in Humans
There is limited evidence in humans for the carcinogenicity of radiofrequency radiation. Positive associations have been observed between exposure to radiofrequency radiation from wireless phones and glioma, and acoustic neuroma.
Cancer in Experimental Animals
There is limited evidence in experimental animals for the carcinogenicity of radiofrequency radiation.
Overall Evaluation
Radiofrequency electromagnetic fields are possibly carcinogenic to humans (Group 2B).
Rationale of the Evaluation of the Epidemiological Evidence
The human epidemiological evidence was mixed. Several small early case–control studies were considered to be largely uninformative. A large cohort study showed no increase in risk of relevant tumours, but it lacked information on level of mobile-phone use and there were several potential sources of misclassification of exposure. The bulk of evidence came from reports of the INTERPHONE study, a very large international, multicentre case–control study and a separate large case–control study from Sweden on gliomas and meningiomas of the brain and acoustic neuromas. While affected by selection bias and information bias to varying degrees, these studies showed an association between glioma and acoustic neuroma and mobile-phone use; specifically in people with highest cumulative use of mobile phones, in people who had used mobile phones on the same side of the head as that on which their tumour developed, and in people whose tumour was in the temporal lobe of the brain (the area of the brain that is most exposed to RF radiation when a wireless phone is used at the ear). The Swedish study found similar results for cordless phones. The comparative weakness of the associations in the INTERPHONE study and inconsistencies between its results and those of the Swedish study led to the evaluation of limited evidence for glioma and acoustic neuroma, as decided by the majority of the members of the Working Group. A small, recently published Japanese case–control study, which also observed an association of acoustic neuroma with mobilephone use, contributed to the evaluation of limited evidence for acoustic neuroma.