Documentation provided by this webpage consists of an excerpt of written comments provided to the City of Naperville, Illinois, as part of a public proceeding conducted by the City of Naperville, Illinois (the City) in March 2013 held pursuant to Public Utility Regulatory Policies Act of 1978. This type of public proceeding is commonly referred to as a “PURPA hearing.” Comments pertain to the Naperville Smart Grid Initiative (NSGI).
In considering an investment in a smart grid system, the associated deployment of smart meters, and an Advanced Metering Infrastructure (AMI), a utility is to consider a number of factors including the societal impact of the investment.
The comments you are about to read make the following assertion:
- Deployment of an Advanced Metering Infrastructure (AMI) may negatively affect the overall health of the residents of the City, especially the vulnerable populations, such as the elderly and lower-income or disabled persons.
The comments submitted to the City of Naperville are provided below. They are an excerpt of the comments only to the extent that the complete document was edited to remove the associated cover letter, some introductory statements, and other information not directly related to the assertion made above.
Introduction
One of the most advertised societal benefits of the smart grid system for the City of Naperville is the “expected lower green house emissions due to energy [usage] reductions.” It is hypothesized that the smart grid system will lead to a “healthier” environment for members of our society to live, work, and breathe. However, for reduced energy consumption to be considered a net societal benefit, it must overcome some potentially significant negative health impacts associated with reduced energy consumption. Have these negative health impacts been considered in the Naperville AMI deployment? To my knowledge, the City of Naperville focuses on the largely hypothetical positive benefits of the AMI, not the more tangible negative risk factors.
I have previously discussed the relevant negative smart grid-related risk factors of privacy, data security, and potentially adverse health effects from radiofrequency (RF) radiation emissions. These factors are relevant for anyone just being a part of the smart grid system, whether or not one participates in associated energy control programs.
If we hypothetically progress to the next step and assume public participation in the energy control programs offered through the AMI, it seems to be assumed by the City that participation in the AMI would have a net positive societal impact. However, an opposite assertion can be made. The most dramatic impact on energy consumption by participating in the energy control programs of the AMI would be in the areas of heating and cooling. The message to consumers is basically to sacrifice personal comfort and quality of life in order to reduce energy consumption for the benefit of the planet. But unfortunately, we normally set the thermostat at a comfortable temperature for a reason; we “feel better” at that temperature. As will be further demonstrated in the paragraphs that follow, thermostat settings go well beyond how we feel. The temperature set points in our homes influence our current and future health status, especially for the most vulnerable and elderly in our society.
The Health Impact Assessment (HIA) of the ComEd AMI Deployment
Much of the supporting information for this discussion is derived from a report issued in April 2012, by the National Center for Medical-Legal Partnership (NCMLP) at Boston Medical Center. The report is entitled, “The Health Impact Assessment (HIA) of the Commonwealth Edison (ComEd) Advanced Metering Infrastructure (AMI) Deployment,” hereafter referred to as the “AMI Health Impact Assessment.”
The entire report is available at the following link:
Health Impact Assessment (HIA) of the ComEd AMI Deployment
Also refer to: http://www.pewtrusts.org/en/multimedia/data-visualizations/2015/hia-map/state/illinois/advanced-metering-infrastructure
The relevance of some information contained in the referenced report may be limited to the ComEd service territory and its specific planned AMI deployment. However, I reviewed the document to extract information that would likely be applicable for all smart grid systems or could at least give perspective to the City’s specific AMI deployment.
I will now generously offer selected quotations from the “AMI Health Impact Assessment”:
“The purpose of this health impact assessment (HIA) is to evaluate the potential health impacts of the deployment of Advanced Metering Infrastructure (AMI) for residential customers in the Commonwealth Edison service territory in Illinois. The purpose of this HIA is not to evaluate whether or not AMI meters should or should not be deployed, but rather to highlight the health and safety aspects of AMI for consideration by the Illinois Commerce Commission (ICC) as it reviews proposed AMI deployment plans.”
“The connection between access to affordable electric service and health has largely gone unacknowledged in debates about AMI deployment.”
“Residential electricity affords light, warmth, and cooling to American homes, and decisions about its use dictate indoor temperature and humidity as well as whether or not alternative sources of energy, such as candles or stoves, are used for light and heat. Consumer decision-making about energy use and equity issues related to energy access shape health.”
“There are many different factors that influence health, from those that are beyond individual control (e.g., age, gender, genetics) to those that are linked to individual behavior (e.g., smoking, drinking, exercising, eating) to structural factors, such as:
- Access to public services and infrastructure (such as education and health care),
- Living and working conditions (such as housing quality and workplace hazards), and
- Social and economic factors (such as social cohesion and neighborhood poverty).
The responses of a population to ambient and changing temperatures reflect a number of factors, including the capacity of the housing infrastructure to concentrate or buffer weather conditions and the degree to which a population, especially vulnerable subgroups, adjust, such as by changing clothing or moderating activity. Impacts can be measured by mortality, emergency room visits and hospitalizations, among others. For example, a series of studies of temperature and mortality rates among U.S. cities finds that deaths increase by 2 to 4 percent per degree Fahrenheit as temperatures climb above a city’s heat threshold and up to 6 percent per degree F with a drop in temperature below the area’s cold threshold (Braga et al., 2001; Medina-Ramon and Schwartz, 2007; Anderson and Bell, 2009). These effects are exacerbated among the very young or very old, minorities and socially isolated individuals. Chronic ailments made worse by exposure include cardiovascular and cerebrovascular disease, respiratory conditions, diabetes, kidney disease, and neurological and movement disorders.”
“Health Outcomes Related to Usage: Health outcomes related to exposure to excessive heat or cold are an important concern in this HIA. The literature on the relationship between temperature exposure and health is voluminous, encompassing retrospective longitudinal observations of mortality differentials by season or weather event (deep freeze, heat wave) over years and decades, case studies of health services utilization during heat waves, and clinical studies detailing the physiological changes that accompany exposure. For the purposes of this HIA, the most relevant studies are those that document indoor temperature exposure, its relationship to energy use and to health and safety outcomes; a much smaller universe of literature makes the link to home energy and very few studies connect temperature exposure directly to energy.”
“Exposure to cold: A meta-analysis of studies linking winter outdoor temp to excess cardiovascular and respiratory disease deaths, for the most part based on data from the United Kingdom, Europe, and New Zealand, concludes that between 30% and 50% of premature deaths in winter reflect exposures to indoor cold (Rudge, 2011, based on Keatinge and Donaldson, 2000 for upper bound and Wilkinson et al., 2001 for lower bound). These otherwise avoidable deaths are associated with lower temperatures in bedrooms and living rooms (adults age 50+) (Eurowinter Group, 1997).”
“Exposure to heat: Recent published summaries of the literature on heat exposure and heat waves highlight dozens of peer-reviewed studies documenting elevated rates of hospitalization and premature deaths. One such review identifies 29 studies where short-term rises in outdoor temperature are associated with greater risk or likelihood of premature death (Basu, 2009).
Another review specifically concerning the experiences of seniors finds 6 peer-reviewed studies where a heat wave or summertime hike in temperature is associated with greater morbidity, and 24 peer-reviewed studies linking heat waves of higher ambient temperature with higher mortality rates (Astroma et al., 2011). Young or advanced age, disabled status (especially a disability that limits mobility), African American ethnic identity, and social isolation or lack of social capital are each indicators of greater vulnerability to adverse impacts related to heat or cold exposure (Bouchama et al., 2007; Kilbourne, 2008; Schwartz. 2005, Medina-Ramon et al., 2007).”
“Chronic Illness and Temperature Exposure: With respect to chronic illness and temperature exposure, various studies have found the following relevant results:
- Heart Disease. Among adults and seniors, both heat and cold are associated with greater risk of hospitalization and premature death from cardiovascular and cerebrovascular (stroke-related) diseases (Alanitis et al., 2008; Medina-Ramon et al., 2006, Ostro et al., 2010, Semenza et al., 1999, Naughton et al., 2002).
- Respiratory Disease. For elders, chronic obstructive pulmonary disorder is made worse by indoor cold: in wintertime, patients whose living rooms are warm (at least 21 degrees C, or approximately 70 degrees Fahrenheit) fewer than nine hours per day have worse respiratory health than those who have at least nine hours of indoor warmth on a daily basis (Collins, 2000; Osman et al., 2008). Children are more than twice as likely to experience respiratory symptoms when they live in cold homes, compared with those who live in warm homes (Marmot Review Team, 2011).
- Diabetes, Kidney Disease, Neurological and Movement Disorders. Heat represents a particular threat for diabetes patients, who are more likely to be hospitalized or die prematurely during a heat wave or non-extreme summer temperatures, as well as those living with kidney disease, who are more likely to be hospitalized for or die from acute renal failure (Schwartz, 2005; Ostro et al., 2010; Semenza et al., 1999, Medina-Ramon et al., 2006; Naughton et al., 2002). Heightened risk for persons with psychiatric disorders or with movement disorders including Parkinson’s have been documented.”
“Age: As described in the preceding section, about 8% of households in census tracts that include ComEd residential customers include children no more than 5 years old, and 11% include an elder at least 65 years of age. At both ends of the age spectrum, thermoregulation of body temperature is more difficult, leaving young children and elders more vulnerable to temperature-related ailments.”
“Social Isolation: Seniors who live independently, especially on limited incomes, are more vulnerable to temperature-related health effects when they lack social supports or connections (defined by social scientists in terms of social capital, a measure of civic relationships and functioning). … Lack of regular social contact can put these residents at greater risk for premature death or illness in the case of a heat wave or the loss of electrical heat in winter.”
“Disability Status: Within ComEd’s service territory, 15.7% of adults report a disabling condition, and 17.2% of households include someone with a disability. Of particular concern are disabilities that limit mobility, or the ability to leave housing conditions that are too hot or too cold; 10.2% of households living in poverty include a member with a mobility-limiting disability and 13.5% of households comprised of seniors include someone with such a disability.”
“Temperature-Sensitive Conditions: Data on the range of chronic ailments affected by temperature are limited. For Illinois counties served by ComEd, 13.7% of adults report their health to be fair or poor, 13.4% of adults report an asthma diagnosis and 13.4% report a child with asthma, 8% of adults report a diagnosis of diabetes, and 28.9% of adults report having high blood pressure, which is a risk factor for heart (cardiovascular) disease and stroke (cerebrovascular disease). Chronic obstructive pulmonary disorder (COPD) and renal (kidney) disease also mean an increased risk of adverse outcomes in the case of exposure to heat or cold, but there are insufficient data to estimate prevalence rates for this population.”
“AMI Pilot Program and Air Quality Benefits: Programs that encourage energy efficiency and conservation can reduce the amount of air pollution from power plants if they reduce the total [emphasis added] consumption of electricity. Demand response programs can also reduce emissions when peak loads are avoided (peak shaving) or when load is shifted in time from higher-emitting peaking power plants to lower-emitting base load or intermediate-load power plants (a condition that does not always obtain, in which case load shifting would increase emissions). … EPRI reported “little evidence” of a reduction in the total energy consumed. A separate analysis of the AMI pilot conducted for ComEd by Black and Veatch estimated that 30,000 MWh of electric generation would be avoided from customer energy efficiency or other voluntary use reductions, after full deployment of AMI to all ComEd customers. This is a very small amount of energy savings [emphasis added] (0.03% of ComEd’s total of 91.1 million MWh in sales in 2010).
The combined reduction in CO2 emissions of 25,000 tons per year, derived from Black and Veatch’s estimates of the benefits of full AMI deployment, would be roughly equivalent to the annual CO2 emissions from roughly 4,400 passenger vehicles or the energy consumed in 2,000 homes. For comparison, the Chicago metropolitan area’s total CO2 emissions have been estimated to be about 40 million tons.”
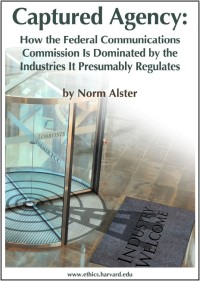
“Non-Ionizing (EMF) Radiation Exposure: Though all consumers may be exposed to some level of radio-frequency radiation in connection with the wireless communication capacity of the AMI digital meters, depending on the physical configuration of meters and the duty cycles, the health impact of these exposures remains unclear. AMI digital meters emit non-ionizing (EMF) radiation as part of their wireless transmission of usage information and operational status between a household and Commonwealth Edison. There is considerable public controversy over the potential and actual health effects of non-ionizing radio frequency radiation to which consumers are exposed by means of wireless transmission.”
“The safety standard regulated by FCC concerns the capacity of radiation to raise the temperature of body tissue (thermal effect), affecting behavior; non-thermal effects have been much more difficult to document.”
“There are very few reports that focus on digital or ‘smart’ meters and their emissions; much of the literature draws on studies of cell phones and microwave transmission towers, which are not the same amount or length of exposure. … There is no scientific consensus about the range and extent of non-thermal health effects linked to non-ionizing radio frequency radiation given off by wireless transmitters and [there is] a need for more research in this area (NRC, 2008).”
“In considering likely exposures for consumers in households with digital meters, a number of factors are relevant, including:
- The distance between the wireless transmitter and the person exposed; the extent of exposure drops off logarithmically or rapidly with increasing distance. … Distance would also reflect the specific configuration of a digital meter or meters, for example, whether household members would be exposed to radiation from a single meter or a row of meters in the case of a multifamily dwelling.
- The duty cycle, or length of time over which wireless transmission takes place; estimates are that digital meters may be transmitting about 50% of the time once automatic meter reading is fully enabled. In addition, digital meters may serve as relays for signals from other digital meters, increasing the total time during which transmissions are occurring.”
“Based on an expert review of studies of cell telephone usage, the World Health Organization’s International Agency for Research on Cancer has labeled EMF radiation possibly carcinogenic to humans (Group 2B); a more comprehensive review is underway. According to the IARC, ‘This category is used for agents for which there is limited evidence of carcinogenicity in humans and less than sufficient evidence of carcinogenicity in experimental animals. It may also be used when there is inadequate evidence of carcinogenicity in humans but there is sufficient evidence of carcinogenicity in experimental animals. In some instances, an agent for which there is inadequate evidence of carcinogenicity in humans and less than sufficient evidence of carcinogenicity in experimental animals together with supporting evidence from mechanistic and other relevant data may be placed in this group. An agent may be classified in this category solely on the basis of strong evidence from mechanistic and other relevant data.’ (WHO/IARC, 2011).”
Summary of Findings/Impacts for the AMI Health Impact Assessment:
“The HIA finds that AMI implementation could result in higher residential energy costs for vulnerable populations. There would be economic incentives for customers to use less electricity when it is most needed for central air conditioning (i.e., critical peak pricing).”
“Significant proportions of residents have characteristics that put them at greater than average risk of adverse health impacts if they have less access to electrical service, or indicate a heightened risk, including difficulties paying for housing, health care, and food; problems heating or cooling their homes due to cost (including a lack of access to central air-conditioning, the single strongest protection against heat-related illness); reliance on electricity for heat or to power medical devices; and substandard housing quality.”
“Fuel-poor households close off parts of their home to reduce energy bills and leave home for part of the day, incurring stress that can lead to criminal activity among teenagers and increased social isolation among adults. Even for seniors who are not low-income, sensitivity to the perceived price of electrical service can influence a decision not to use air-conditioning during summer heat.”
“Vulnerable populations are subject to a number of risks in their lives due to their economic status and these risks could be exacerbated as a result of AMI deployment.”
“The HIA also found that customers faced with making decisions regarding trade-offs, especially trade-offs that would put their health and safety at risk, experienced greater stress related to paying utility bills when compared with energy assistance recipients across the nation. AMI alone is not the ‘prime’ mover of causing underlying fuel poverty, but can exacerbate it with potential health consequences.”
“Non-ionizing, (EMF) radiation emitted by AMI raises questions about long-term, adverse health impacts but the extent to which AMI will increase residential exposure to non-ionizing radiation is unknown.” [Note: My commentary on this statement would be that it supports a position of prudent avoidance of additional RF radiation in the home based upon “questions about long-term, adverse health impacts” and “unknown” extent of increased residential exposure to non-ionizing radiation. “Unknown,” of course, in no way demonstrates safety.]
Health Impact Implications for an AMI Deployment in Naperville
Based upon the type of information presented in the preceding section, it can be postulated that that the deployment of the City’s AMI may actually have an overall negative impact on the health of the residents of the City, especially the vulnerable populations, such as the elderly and lower-income or disabled persons.
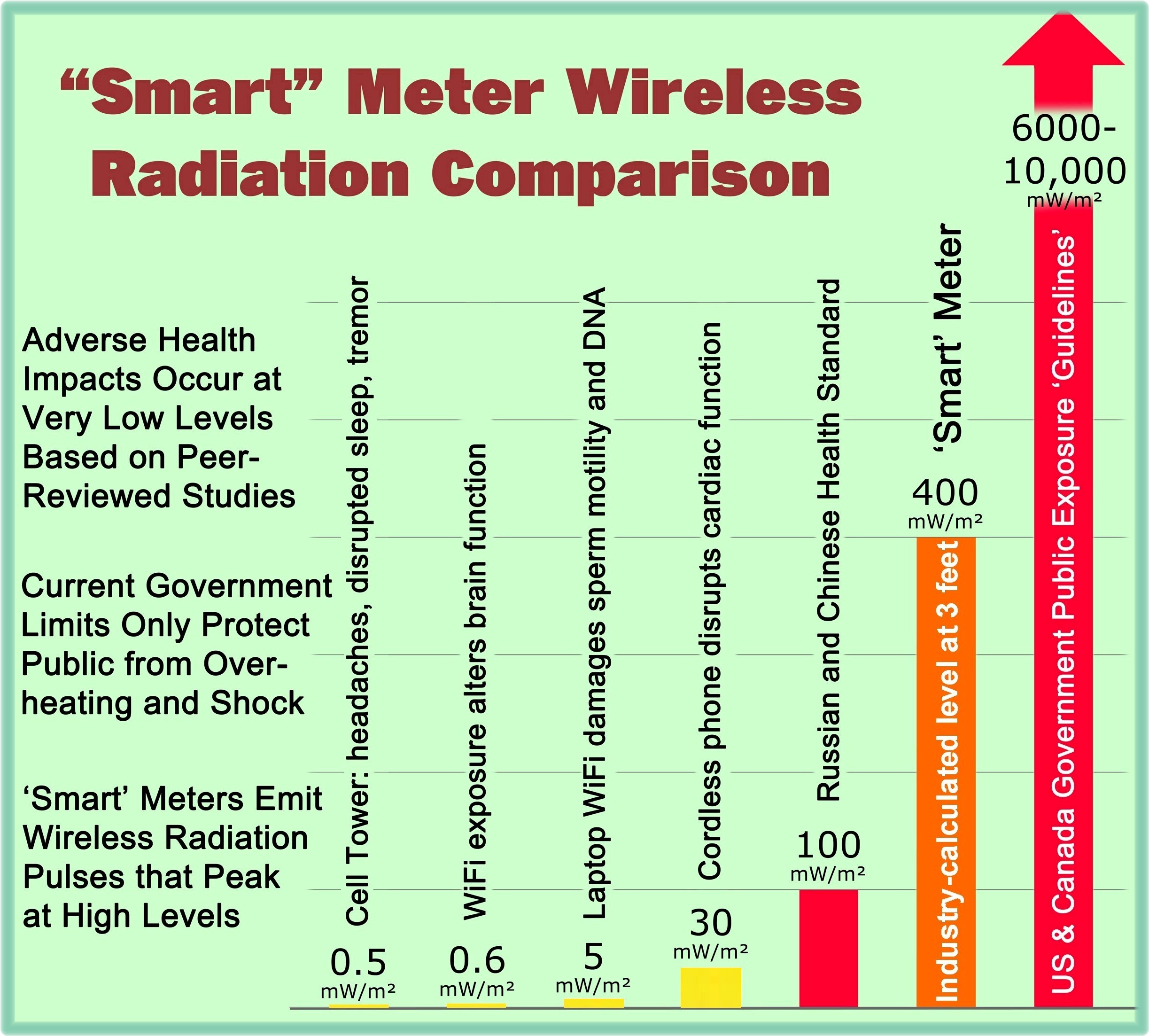
The “AMI Health Impact Assessment” mentions that the “AMI technology itself” may have health impacts related to the RF emissions from the wireless smart meters and other elements of the smart grid system. But at least in the context of this report, one of the main conclusions of the “AMI Health Impact Assessment” is that temperature-sensitive health conditions are made worse by exposure to heat or cold.
Below is an excerpt from a table in the report that attempts to quantify some of the types of conditions made worse by exposure to heat or cold.
In Naperville, how could the deployment of an AMI result in an increased exposure of its residents to heat or cold? The principal mechanism would include the following:
- Residents and consumers living on fixed incomes and constrained budgets, including vulnerable populations, would feel pressured (through marketing and incentives) to participate in energy control and pricing programs offered by the City that charge different rates at certain times of the day or require the consumer to reduce energy consumption in order to receive a discounted rate. This behavior will result in an under-usage of electricity resulting in extremes for the indoor temperatures of affected consumers. It has been shown that exposure to temperatures outside of a “moderate range” increases the likelihood of hospital emergency department visits, hospitalizations, and premature death.
[Note: The content for the above paragraph is derived from direct testimony of Megan Sandel, MD, MPH, before the Illinois Commerce Commission on May 11, 2012, on behalf of the AARP and the People of the State of Illinois.]
In return for the tangible negative health effects associated with the AMI, we would in turn receive the potential miniscule, if any, benefits of improved air quality associated with air pollution released from power plants used to generate electrical energy. Based upon the information in the “AMI Health Impact Assessment,” these benefits would likely be too small to ever measure.
Conclusions
Regarding … Smart Grid Investments, the City must adequately address the factors of invasion of privacy, data security, RF emissions, consent issues and opt-out fees related to imposing digital smart meter technology on its customers, and [now] finally, the overall health impact of an AMI deployment on its residents.